
Abstract
Background
Overuse and abuse of antibiotics resulted in emergence of multidrug-resistant organisms (MDRO), increased rates of invasive candidiasis, prolonged hospital stay, NEC (Necrotizing enterocolitis), LOS (Late onset sepsis) or death. Restriction of the prescription, switching to a narrower spectrum and stopping antibiotics when not needed are some of the major approaches to antibiotic stewardship.
Methods
We identified restricted antimicrobials and devised an antimicrobial justification form. Clinicians needed to fill the form before prescribing restricted antimicrobials thereby comparing the antimicrobial usage pattern before and after the introduction of form. Babies enrolled before the introduction of the justification form were labelled as Group 1, and as Group 2 after justification form. The HIC (hospital infection control) staff nurse paid daily visits to NICU to monitor number of babies started on restricted antibiotics and whether the forms were duly filled or not. Any lag would be intimated to the Head HIC team for rectification. Any change of antibiotic within the restricted group also warranted justification. Culture report notified within 48 – 72 hrs so as to facilitate the stoppage of antibiotics in case of negative culture.
Results
There was a statistically significant reduction in the usage of restricted antimicrobials in the Group B as compared to Group A 150 (40.54%) vs 190 (49.35%) (p = 0.01). There was a statistically significant increase in the % of babies de-escalated from high end antimicrobials in Group B as compared to Group A 90 (60%) vs 56 (29.47%) (p = <0.0001). Duration of restricted antimicrobials reduced from 13.78 ± 2.7 days in Group A to 9.9 ±1.8 days in Group B (p = <0.0001). No difference in the number of babies started on any antibiotic between both the groups (p = 0.1).
Conclusion
Introduction of the antibiotic justification form as a part of antimicrobial stewardship program resulted in an overall reduced usage of restricted antimicrobials along with rapid de-escalation.
Author Contributions
Academic Editor: Jennifer Cole, Infection Prevention at Avanti Hospitals, LLC, Los Angeles, CA
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 S V N S Sowjanya
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Introduction of antibiotics has transformed the practice of medicine and have significantly reduced the morbidity and mortality across all ages. In neonates there are certain specific challenges when we talk about sepsis and prescription of antibiotics. The signs and symptoms of sepsis in neonates are non-specific, sampling for blood cultures may not be feasible at all times, culture positivity rates are low and when cultures grow coagulase-negative staphylococcal (CoNS) species, distinguishing between infection and colonization or contamination becomes difficult. Still antibiotics continue to be the most commonly prescribed medications in neonatal intensive care units (NICUs)1. We have faced the wrath of overuse or abuse of antibiotics in the form of sepsis outbreaks in NICU’s2, 3, 4with multidrug-resistant organisms (MDROs), increased rates of invasive candidiasis5, 6, 7, increases incidence of Necrotizing enterocolitis (NEC) even in late preterm and term neonates and so on. NICU becomes a unique zone compared to the rest of the hospital in view of the tiny, fragile and immature patients it caters, who are immunologically and physiologically different compared to adults and older children. Antimicrobial stewardship (AMS), as defined by the Infectious Diseases Society of America (IDSA), includes interventions targeted toward the improvement and monitoring of appropriate antimicrobial use by selecting the most optimal drug regimen, including the type of drug used, the dose, duration of therapy, and route of administration8. Cutting down on the overuse appears to be the most effective way to implement AMS9. But somehow this approach has not been studied much10. We studied the impact of an intervention directed at cutting down the overuse of restricted antimicrobials.
Methods
This prospective study was conducted in a tertiary level 3 neonatal intensive care unit in Chennai, India from May 2015 to June 2016. We divided the study period into 2 eras. Era 1 from May 2015 to November 2015 and Era 2 from December 2016 to June 2016 after the introduction of ‘Antibiotic Justification Form’ (Figure 1). Babies were prospectively enrolled after consent. Babies admitted in Era 1 were labelled as Group A and those admitted in Era 2 were labelled as Group B. Institutional ethics committee approval was taken prior to the start of the study (IRB-MCH/18/2015). The antibiotic justification form was devised after discussion with the hospital infection control (HIC) team based on the overall culture positivity rates, microbiological spectrum of organisms and the antimicrobial sensitivity. The form needed details like diagnosis, empirical or definitive therapy with justification and signature of the consultant with date and time. The form was introduced on November 15, 2015 and the nurses and doctors were trained for 15 days in its usage. The form had to be filled within 24 hours of starting a restricted antimicrobial along with the justification and counter signed by the consultant. The HIC staff nurse visits NICU daily to monitor number of babies started on restricted antibiotics and whether the forms are duly filled or not. Any lag would be intimated to the Head HIC team for rectification. The culture report is documented in 48-72 hrs so as to stop the antibiotics in case of a negative culture. The HIC staff nurse would insist the treating doctor on de-escalation of restricted anti microbials based on the culture reports and clinical scenario if not done already. Any change of antibiotic within the restricted group also warranted justification. Monthly review of the forms was done by the hospital infection control (HIC) committee.
Figure 1.Antibiotic justification form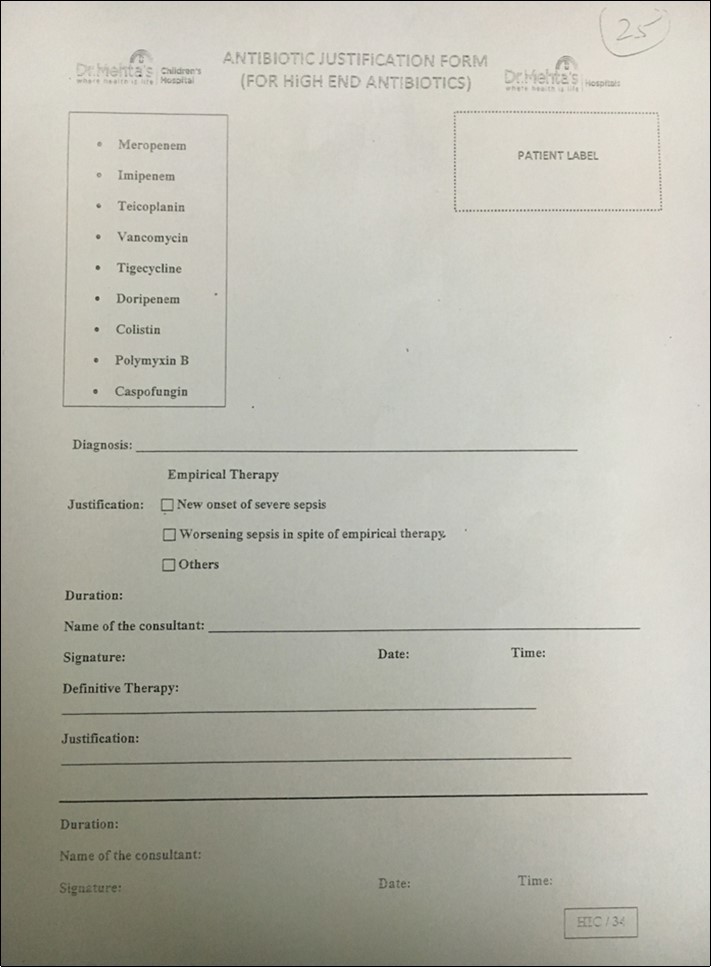
Antibiotic Policy
Era 1
The first line antibiotics were Ampicillin, Piperacillin - tazobactum and Amikacin. The duration of antibiotics was 7 – 10 days for empirical therapy and 14 days for culture positive sepsis. There was no restriction of usage of high-end antimicrobials and it was purely based on the discretion of treating physician.
Era 2
The first line antibiotics were Ampicillin, Piperacillin - tazobactum and Amikacin. Meropenem, Imipenem, Teicoplanin, Vancomycin, Tigecycline, Doripenem, Colistin, Polymixin B, Caspofungin were labelled as high-end antibiotics or restricted group. Prescription of such high-end antimicrobials needed filling of the antibiotic justification form along with the reason to start and signature of the consultant. De-escalation of the restricted anti-microbial to be done as early as possible. The duration of antibiotics was 5 – 7 days for empirical therapy and 10 – 14 days for culture positive sepsis.
Statistical Analysis
Our estimated incidence of use of restricted antimicrobials prior to the study was around 45%. In order to reduce the use of restricted antimicrobials from 45% to 25% with alpha error 0.05 and power 90%, 398 cases and 398 controls would be required. Student t test and chi square test used for continuous and categorical variables respectively. Comparison of means and proportions used wherever appropriate. Relative risk and mean difference with 95% confidence intervals calculated. P value less than 0.05 was considered statistically significant.
Results
429 babies were admitted in Era 1 whereas 428 babies were admitted in Era 2. The two groups were comparable in terms of gestational age, diagnoses, mortality and sepsis rates (Table 1). 190 babies (49.35%) received restricted antimicrobials in the Era 1 compared to 150 babies (40.54%) in Era 2 (p = 0.01). The total duration of restricted antimicrobials significantly reduced from 13.78 days to 9.9 days in Era 2 (p = <0.0001). 56 babies (29.47%) were deescalated from restricted group to first line antibiotics in Era 1 compared to 90 babies (60%) in Era 2 (p = <0.0001). The duration of first line antibiotics also significantly reduced from 9.06 days to 4.8 days (p = <0.0001). However, there was no difference number of babies started on any antibiotic in both the groups (p = 0.1). The outcomes are summarized in Table 2. We analysed the usage of our first line antibiotics in both the eras (Table 3). The usage of Amikacin was significantly reduced in Era 2 (p = 0.01). Table 4 shows the reasons for usage of restricted antimicrobials. The most common cause for usage of high-end antibiotics in Group A was clinician’s decision (p = <0.0001) whereas in Group B it was worsening sepsis in spite of empirical therapy (p = <0.0001).
Table 1. Comparison of baseline characteristics between Group A and B| Characteristic | Group A (May 2015 – November 2015) | Group B (December 2015 – June 2016) | P value |
| Total admissions* | 429 (50.05%) | 428 (49.94%) | 0.97 |
| Number of Outborn babies* | 316 (73.66%) | 324 (75.7%) | 0.55 |
| Male* | 235 (54.77%) | 240 (56.07%) | 0.7 |
| Gestational Age** (Weeks) | 34.38 (0.9) | 34.33 (0.7) | 0.36 |
| Ventilated* | 90 (20.97%) | 81 (18.93%) | 0.45 |
| CPAP* | 66 (15.38%) | 58 (13.55%) | 0.44 |
| RDS* | 95 (22.14%) | 85 (19.86%) | 0.41 |
| MAS* | 20 (4.66%) | 19 (4.44%) | 0.88 |
| Asphyxia* | 22 (5.13%) | 19 (4.44%) | 0.63 |
| Culture Positive Sepsis* | 18 (4.19%) | 14 (3.27%) | 0.48 |
| Surgical* | 8 (1.86%) | 6 (1.4%) | 0.59 |
| Deaths* | 10 (2.33%) | 12 (2.8%) | 0.66 |
| Outcome | Group A (N = 429) | Group B (N = 428) | Relative risk/Mean difference (95%CI) | P value |
| Number of babies on restricted group* | 190 (49.35%) | 150 (40.54%) | 8.81 (1.7 to 15.7) | 0.01 |
| Total duration of restricted group (Days)* | 13.78 (2.7) | 9.9 (1.8) | -3.88 (-4.19 to -3.57) | <0.0001 |
| Number of babies started on any antibiotic* | 385 (89.74%) | 370 (86.44%) | 3.3 (-1.2 to 7.81) | 0.1 |
| Number of babies deescalated from restricted group* | 56 (29.47%) | 90 (60%) | 30.53 (20 to 40) | <0.0001 |
| Total duration of first line antibiotic (days)** | 9.06 (2.1) | 4.8 (1.6) | -4.26 (-4.51 to -4) | <0.0001 |
| Group A(N = 429) | Group B(N = 428) | Relative risk/Mean difference (95%CI) | P value | |
| No antibiotic* | 44 (10.26%) | 58 (13.55%) | 3.29 (-1.21 to 7.8) | 0.14 |
| Empirical 1st line* | 195 (50.65%) | 175 (47.29%) | 3.36 (-3.7 to 10.4) | 0.36 |
| Ampicillin* | 45 (23.07%) | 40 (22.85%) | 0.22 (-8.4 to 8.7) | 0.96 |
| Piperacillin Tazobactum* | 175 (89.74%) | 155 (88.57%) | 1.17 (-5.2 to 7.7) | 0.72 |
| Amikacin* | 190 (97.44%) | 160 (91.43%) | 6.01 (1.34 to 11.3) | 0.01 |
| Group A(N = 190) | Group B(N = 150) | Relative risk/Mean difference (95%CI) | P value | |
| Empirical 2nd line* | 172 (90.53%) | 136 (90.66%) | 0.13 (-6.8 to 6.7) | 0.96 |
| New onset severe sepsis* | 40 (23.26%) | 30 (22.06%) | 1.2 (-8.8 to 10.9) | 0.8 |
| Worsening sepsis in spite of empirical therapy* | 68 (39.53%) | 90 (66.17%) | 26.24 (15.07 to 37.43) | <0.0001 |
| Clinician’s decision* | 64 (37.21%) | 16 (11.76%) | 25.45 (15.63 to 34.56) | <0.0001 |
| Definitive therapy* | 18 (9.47%) | 14 (9.34%) | 0.13 (-6.8 to 6.7) | 0.96 |
Discussion
In our study, we observed that introduction of ‘Antibiotic Justification Form’ has the potential of restricting the use as well as the de-escalation of high-end antimicrobial agents. As both the groups were comparable in terms of demographic profile and disease spectrum and severity, the reduction in the initial usage and later de-escalation of these antimicrobials can be attributed to the intervention. There was a more stream lined approach to check the antibiotic usage at multiple levels at the same time creating more accountability, responsibility and awareness among the clinicians.
We have restricted only to sepsis because antimicrobial usage is directly related to this condition and hence would give us a clear picture on the antibiotic overuse or abuse. As a unit we do not routinely start antibiotics in respiratory, neurological morbidities, instead only when there is a clinical or laboratory evidence of sepsis. We do not deal with oncology cases and post-operative babies are still on first line antibiotics unless any complications
A study by McCarthy et al11 involved a prospective audit to assess the compliance with antimicrobial guidelines. The intervention included an electronic prescribing unlike ours which was a manual filling form. There was a significant overall reduction in the primary outcome of DOT (days of antibiotic therapy)/1000 patient days from 572 to 417 DOT. This represents a 27% reduction in total antibiotic use as compared to 8.81% reduction in our study. Treatment courses >5 days for culture negative sepsis were reduced from 46.5 DOT to 7 DOT. We did not measure the outcome in terms of DOT.
The SCOUT (Surveillance and Correction of Unnecessary Antibiotic Therapy) study is an observational study conducted by Cantey et al12 in USA. Antibiotic use in infants admitted to the neonatal intensive care unit was monitored and analysed over a period of 9 months compared to 1 year in our study. The intervention was electronic medical record to stop antibiotics after 48 hrs. There was an overall decrease of 27% in the antibiotic usage which was higher compared to our study (8.81%).
In a study by Mongkolrattanothai113et al, a prospective audit and feedback on infants on broad-spectrum antibiotics was conducted weekly. Construction of NICU-specific antibiogram to guide empiric therapy decisions, development of the standardized algorithms of early- and late-onset sepsis with guidance on choices and duration of antimicrobial therapy for common infectious syndromes, and prescriber education were implemented as a part of stewardship efforts. This study was more of a QI involving many interventions directed at multiple levels unlike our study which was focusing on the impact of one intervention i.e, antibiotic justification form.
Naeem et al14 implemented antimicrobial stewardship program and also conducted a retrospective analysis of antibiotic usage in the pre implementation era. The details of ASP are clearly mentioned in the study. They noticed a 30% decrease in the antibiotic usage (DOT/100o patient days). They also noticed a reduction in mortality and NEC rates which we did not study.
In an observational double cohort study conducted by Astorga et al15, they implemented an automatic 48 hr stop order which resulted in reduction of total doses given per patient by 35% and doses per patient-day by 25%.
Thampi et al16, conducted antibiotic stewardship program rounds five mornings a week with the NICU medical team. The overall antibiotic use and use of narrow spectrum reduced. There was no change in duration of antibiotics in culture negative sepsis. And there was an increased used of cefotaxime.
Priti jagdishbai tank et al117, conducted a prospective audit of antibiotics every day for 5 days whether antibiotics are stopped, continued or changed based on clinical condition of the neonate. They found that overall documentation and investigations to confirm infection was poor. The continuation of antibiotics was inappropriate. To improve documentation, availability of a checklist on admission is recommended.
In order to implement AMS successfully, we need prospective surveillance systems guided towards clinical decisions18. Such studies are still lacking in NICU’s.
Our study is one such prospective surveillance, where we were able to curtail the indiscriminate use of antibiotics and reduce the duration of the antimicrobial therapy after introduction of a simple intervention like “antibiotic justification form”.
Our study shows that antibiotic stewardship in the neonatal intensive care unit is feasible and can be achieved safely. Antibiotic stewardship interventions in neonatal unit need collaboration and combined team effort from Neonatologists, Nursing staff, Microbiologists and Hospital infection control team. There is no fixed formula or method for the implementation of antibiotic stewardship program and it can be tailor made to the needs and clinical scenario of the local population in order to improve the success.
There are certain limitations in our study. Most of the previous studies expressed the outcome as DOT (days of therapy)/1000 patient days. Impact of the intervention on antimicrobial sensitivity pattern was not studied. We did not analyse the impact of antibiotic justification form on neonatal outcomes like Mortality, NEC, Duration of hospital stay and Cost.
Conclusion
Introduction of “antibiotic justification form “ results in reduced usage, rapid de-escalation and reduced duration of higher end antibiotics attributed to the awareness created among the clinicians. This is a simple, easy and cost-effective way of implementing antibiotic stewardship in NICU’s yet showing promising results.
References
- 1.Clark R H, Bloom B T, Spitzer A R, Gerstmann D R. (2006) Reported medication use in the neonatal intensive care unit: data from a large national data set. , Pediatrics; 117, 1979-87.
- 2.Lesch C A, Itokazu G S, Danziger L H, A Weinsten R. (2001) Multi-hospital analysis of antimicrobial usage and resistance trends. Diagn Microbiol Infect Dis. 41, 149-54.
- 3.Singh N, Patel K M, Leger M M, Short B, Sprague B M et al. (2002) Risk of resistant infections with Enterobacteriaceae in hospitalized neonates. Pediatr Infect Dis J. 21, 1029-33.
- 4.P de Man, Verhoeven B A, Verbrugh H A, Vos M C, JN Van den Anker. (2000) An antibiotic policy to prevent emergence of resistant bacilli.Lancet.355:. 973-978.
- 5.Cotten C M, McDonald S, Stoll B, Goldberg R N, Poole K et al. (2006) The association of third-generation cephalosporin use and invasive candidiasis in extremely low birth-weight infants. , Pediatrics; 118, 717-722.
- 6.Lee J H, Hornik C P, Benjamin DK Jr, Herring A H, Clark R H et al. (2013) Risk factors for invasive candidiasis in infants >1500 g birth weight. , Pediatr Infect Dis J; 32, 222-226.
- 7.Saiman L, Ludington E, Dawson J D, Patterson J E, Wiblin R T et al. (2001) Risk factors for Candida species colonization of neonatal intensive care unit patients. , Pediatr Infect Dis J; 20, 1119-24.
- 8. (2012) Society for Healthcare Epidemiology of America; Infectious Diseases Society of America; Pediatric Infectious Diseases Society. Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology. of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Control Hosp Epidemiol 33(4), 322-327.
- 9.Chassin M R. (2013) Improving the quality of health care: what’s taking so long? Health Aff (Millwood). 32(10), 1761-1765.
- 10.Korenstein D, Falk R, Howell E A, Bishop T, Keyhani S. (2012) Overuse of health care services in the United States: an understudied problem. Arch Intern Med. 172(2), 171-178.
- 11.McCarthy K N, Hawke A, Dempsey E M. (2018) Antimicrobial stewardship in the neonatal unit reduces antibiotic exposure. Acta Paediatr. 1716-1721.
- 12.Joseph B Cantey.Reducing unnecessary antibiotic use in the neonatal intensive care unit (SCOUT): a prospective interrupted time-series study. The Lancet Infectious Diseases, Volume 16. , Issue 10, 1178-1184.
- 13.Mongkolrattanothai Kanokporn, Chin Steven, Srikumar Nair, Lin Ting-Yi, Holmen Jenna et al. (2016) . Antimicrobial Stewardship in the Neonatal Intensive Care Unit (NICU): Building and Sustaining the Effective Collaboration, Open Forum Infectious Diseases, Volume 3, Issue suppl_1, 1 .
- 14.Naeem Fouzia.Mohammad Nael Mhaissen, Brenik Kuzmic, Ashley Clark. (2017).Michelle Ruiz and Indira Chandrasekar. Antimicrobial Stewardship Program in a Tertiary Neonatal Intensive Care Unit. Open Forum Infect Dis. Fall;4(Suppl1): 269
- 15.Astorga M C, Piscitello K J, Menda N, Ebert A M, Ebert S C et al. (2019) Antibiotic Stewardship in the Neonatal Intensive Care Unit: Effects of an Automatic 48-Hour Antibiotic Stop Order on Antibiotic Use. J Pediatric Infect Dis Soc. 8(4), 310-316.
- 16.Thampi N, Shah P S, Nelson S, Agarwal A, Steinberg M et al. (2019) Prospective audit and feedback on antibiotic use in neonatal intensive care: a retrospective cohort study. , BMC Pediatr 19, 105.