
A Tandem of Rare Complications Due to Stent Infection
Abstract
This report details sequential rare complications arising from a vascular stent infection. Clinical course, microbiology, and imaging are outlined, with emphasis on early recognition and multidisciplinary management. Lessons for device surveillance and antimicrobial stewardship are highlighted.
Author Contributions
Academic Editor: Raul Isea, Fúndacion Institúto de Estúdios Avanzados, Hoyo de la Púerta, Barúta, Venezúela
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2023 Inga Botchorishvili, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
In spite of advanced interventional equipment and procedural technique an iatrogenic complications still exists with associated morbidity and mortality 1. There are a lot of type of complications but some of them are significantly serious.
Approximately 5 million percutaneous coronary interventions (PCIs) are performed worldwide annually. Stent-related complications occur at a fairly low rate, but they are a major concern for public health. Among these complications, stent thrombosis (ST), with 5–45% mortality and a 15–20% recurrence rate at 5 years, is the most relevant one 2, 3. Implantation of medical devices represents one of the most important risk factor for nosocomial infections, but it is rarely followed by coronary wall injury 5
Case presentation
An 46-year old non-diabetic mail without history history of coronary artery disease 08.06.2020 was admitted to the cardiology department of Bokhua Memorial Cardiovascular Center ,with diagnoses of unstable angina (UA). Coronary angiography revealed 80% stenosis in medial segment of Left Anterior Descenting Artery (LAD). One bare metal stent was implanted in the stenotic segment (see Figure 1). The procedure was performed sucssesfully , without any procedure-related complications. After stent placement at hospital patient remaind simptom free. Heamodinamic parameters were stabile and he was discharged from hospital with appropriate prescription.
Figure 1.(08.06.2020) A. Medial stenosis in LAD. B. Stent implantation. C. Final result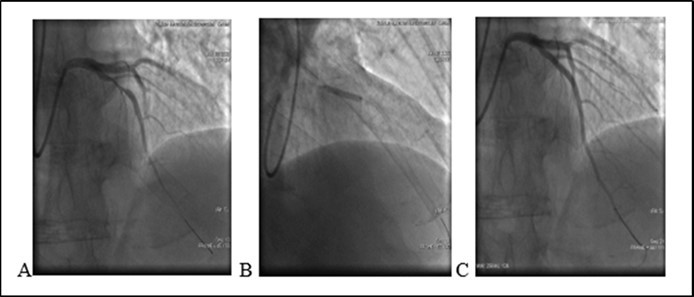
After six days from the PCI a patient was referred to an outpatient clinic with a fever of unknown origin 39.4 C0 . SARS CoV-2 Real-Time PCR was negative. No previous infective disease, fever or angina was reported. A mild elevation of leukocytes was observed 11.2 x10`3/μ L (N 4-10). According to patient information without a clear diagnoses he received empiric wide an antibiotic treatment with azithromycin 500 mg q. d. Our prescription was not changed. After antibiotic administration a body temperature had regulated, it was 36.6 C0.
After angioplasty two weeks later (20.06.2020) 13:25 Pm the patient presented severe chest pain and he was readmited again in the same institution with diagnosis: Coronary artery disease. ST segment elevation MI. Arterial Hypertension I (ESH/ESC). Coronary artery stenting . (LAD 1 Bare Metal Stent (BMS) 08.06.2020).
On ECG : HR 78 . Sinus rythm. ST segment elevation I, aVL, V1- V5 (2mm at the J-point). Q wave in V2-V4 leads. T/A 180/70 mm Hg. Patient refused missing of presribed medications. Due to severe chest pain, ECG data and haemodynamic instability an urgent PCI was performed. It revealed a stent thrombosis in LAD - early stent thombosis (1). Circumflex Coronary artery (CX) and Right Coronary artery (RCA)- without significant changes (see Figure 2).
Figure 2.(20.06.2020) .A. Occluded stent due to early thrombosis (red arrow). B.C Balloon angioplasty and stenting. D. Final result.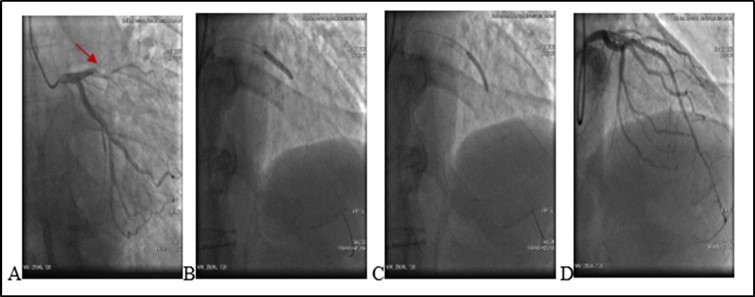
After administration of a 180 mg loading dose of ticagrelor and an intravenous bolus of 10.000 units heparin, left main coronary artery was cannulated with a 6F EXB4 guiding catheter and a 0.014’’ floppy guide wire was advanced in LAD. Coronary artery recanalisation performed successfully. After baloon angioplasty with 3.0X12 mm baloon-catheter, in proximal and medial segments intraluminal filling defect was observed – reduced contrast dencity and heziness and two BMS were overlaped - 3.5X24 mm and 3.0X24 mm respectively. Postdilation was performed at the end of the procedure.TIMI score was 3. Procedure performed without any techincal complication during coronary intervention. Patient was stable and he was transferred to the Intensive Care Unit.
Transthoracic echocardiography images revealed mild left ventricular hypertrophy; grade I diastolic dysfunction, left ventricular regional wall motion abnormality (anterior and anterolateral wall, apical and septo/apical hypo/kinesis) and mild tricuspid and mitral regurgitation. EF-48%. The blood cultures were negative for any bacteria.
21.06.20 05:03 Am the patient complained chest pain. A drop in blood pressure and bradycardia was noted. T/A 80/60 mm Hg. There was no changes on echocardiography. No pericardial separation. No ST segment changes on ECG . Due to hemodynamic instability we decided to repeat a coronary angiography and it again revealed a medial segment stent thrombosis in LAD with multiple extravasations at proximal and medial segments Type III and II (see. Figure 3) -late perforation of coronary artery. At proximal segment pericardial hemorrhage provided pericardial hematoma with diameter 9-10 mm. At medial were visualized. During coronary angiography a patient’s condition deteriorated. Blood pressure dropped to T/A 60/40 mm Hg. A cardiac tamponade developed because of blood leak into pericardial space. A 3 mm balloon was inflated immediately in the site of rupture, with complete occlusion of vessel, stopping of a blood flow in the LAD and termination of extravasation into the pericardial space.
Figure 3.A. (21.06.2020) Second acute stent thrombosis and perforation Type III and II (red arrows) B. Balloon inflation in the site of rupture (red circle).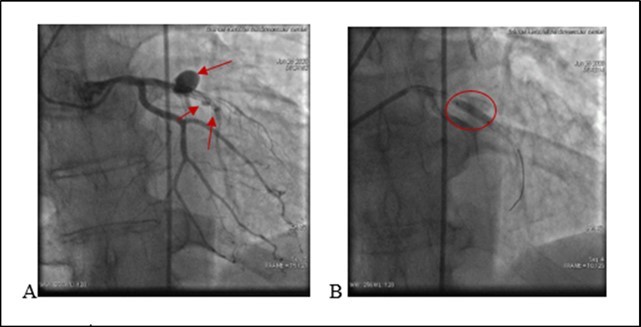
Deployment of covered stents was not purposeful due to highly suspected infection. A decision was made for urgent surgical treatment. A patient was urgently transferred to a cardiac operation theater surgical department with inflated balloon to eliminate a blood leakage in the pericardium. Ligating the coronary artery with removing stents, subsequent bypass grafting was performed, with removal of 500 ml of coagulated blood from the pericardial space. Post-surgery period remained stable. Leukocytes - 14.24 x10`3/μ L (N 4-10). A Pseudomonas Aeruginosa (multirresistent) - was positive after coronary wall tissue histomorphological examination. During hospitalization developed renal insufficiency.
13.07.2020 A patient was discharged with appropriate prescription and recommendations.
Discussion
This case presentation describes a rare infection-related complication of PCI, subsequent and likely causal complications, stent thrombosis followed by coronary artery perforation around the stent.
After six days from initial PCI a patient developed fever without any cardiac symptom. At that time the fever presumably was bacterial origin and lately, after surgery coronary tissue histomorphological examination revealed a positive Pseudomonas Aeruginosa, which was responsible for coronary stent infection.
At early stage of disease empiric antibiotic treatment changed a picture of nosocomial infection. Pseudomonas Aeruginosa initiated infection process around the stent resulted in partial destruction of the arterial wall and stent thrombosis. The first thrombosis was early ST 4. Coronary artery stenting with two overlapping stents was performed in the site of thrombosis. After several hours from the second PCI procedure developed the second acute stent thrombosis and coronary artery perforation. As mentioned above after first stent thrombosis balloon and stent delivery, inflation and influence of mechanical forces destroyed the infected arterial wall integrity and another rare complication had developed at this patient. It was a device induced CAR of infected arterial wall. During angioplasty procedure device-related CAR is rare 14. Current evidence base is limited to small series and the prevalence of these complications (CAP and CAR) is controversial and varies from 0.1% and 3% 15, 16, 17. In discussed case the main source of perforation was infection.
The most intriguing in this case was fever of unknown origin which generally is associated with infection. After initial PCI etiology of developed fever was bacteremia, probably from stent or device contamination. Symptoms of stent infection present days to weeks after the initial PCI 6, however in literature a late coronary stent infection is described 5. Very limited number of PCI-associated coronary stent infections have been reported since 1993 in literature 21. Some of studies revealed the most commonly involved microorganisms: staphylococcus aureus, coagulase-negative staphylococci and group B streptococci. Several study data suggest that clinically significant bacteremia represents an extremely rare complication of cardiac catheterization and the low number of documented coronary stent infection is presented. 7, 8, 9, 10, 11, 12 Due to bacteremia may also develop coronary artery aneurysm and infective endocarditis 13, 14, but none of them were observed in discussed case. Outcome and prognosis of both complications are very poor 18, 19, 7.
Conclusion
This case presentation describes a rare infection-related complication of PCI, subsequent and likely casual complications, stent thrombosis followed by coronary artery perforation around the stent. Also it is a demonstration that the fever manifestation must be considered in the differential diagnosis during one or two weeks after initial PCI. Diagnosis is based on positive blood cultures and is helpful to manage treatment strategy. Infected coronary artery wall represents a high risk of further procedure related complications.
Ethical disclosures
The authors declare that no experiments were performed on humans or animals for this study.
References
- 1.Ellis S G, Ajluni S, Arnold A Z, Popma J J, Bittl J A et al. (1994) Increased coronary perforation in the new device era. Incidence, classification, management, and outcome. , Circulation 90(6), 2725-30.
- 2.Gori T, Polimeni A, Indolfi C, Raber L, Adriaenssens T et al. (2019) Predictors of stent thrombosis and their implications for clinical practice. , Nat. Rev. Cardiol 16, 243-256.
- 4.Erik C, Grove L, Steen Dalby Kristensen. (2007) FESC Stent thrombosis: definitions, mechanisms and prevention. An article from the e-journal of the ESC Council for Cardiology Practice. 5(32).
- 5.Gonda Elizabeth, Allyson Edmundson BA, RN B S, Mann Tift, Late M.Coronary Stent Infection: A Unique Complication after Drug-Eluting Stent Implantation.
- 7.Kaufman B A, Kaiser C, P fisterer ME, Bonetti P O. (2005) Coronary stent infection: A rare but severe complication of percutaneous coronary intervention. Swiss Med Weekly. 35, 483-487.
- 8.Banai S, Selitser V, Keren A, Benhorin J, Shitrit O B et al. (2003) Prospective study of bacteremia after cardiac catheterization. , Am J Cardiol 92, 1004-7.
- 9.Grewe P H, Machraoui A, Deneke T, Muller K M. (1999) Suppurative pancarditis: A lethal complication of coronary stent implantation. , Heart 81, 559.
- 10.Liu J C, Cziperle D J, Kleinman B, Loeb H. (2003) Coronary abscess: A complication of stenting. Catheter Cardiovasc Interv.58:. 69-71.
- 11.Bangher M, Lava P, Baccaro J. (2003) Coronary stent infection: Case report and definition. , Rev Esp Cardiol 56, 325-326.
- 12.MQ Narins CR Le. (2007) Mycotic pseudoaneurysm of the left circumflex coronary artery: A fatal complication following drug-eluting stent implantation. Catheter Cardiovasc Interv.69:. 508-512.
- 13.Leroy O, Martin E, Prat A. (1996) Fatal infection of coronary stent implantation. , Cathet Cardiovasc Diagn 39, 168-170.
- 14.Bouchart E, Dubar A, Bessou J P. (1997) Pseudomonas aeruginosa coronary stent infection. Ann Thorac Surg. 64, 1810-1813.
- 15.Ismail Dogu Kilic.Yusuf IA, Serhat BY.(2013). Coronary artery perforations: Four different cases and a review. Sociedade Portuguesa de Cardiologia. 32(10), 811-815.
- 16.Oliver P Guttmann, Daniel A Jones.PhD; Ankur Gulati, MD; Tushar Kotecha, MBBS; Prevalence and outcomes of coronary artery perforation during percutaneous coronary intervention.EuroIntervention 2017; 13:. 595-601.
- 18.Kinnaird Tim, Chun S K, Evangelos K, Nicholas O, Peter L et al. (2006) Determinants, and Outcomes of Coronary Perforation During Percutaneous Coronary Intervention in the United Kingdom Between.
- 19.Eeckhout Eric, Rodney De Palma.Coronary Perforation An Inconvenient Comlication. , JACC:Cardiovascular Interventions 4(1), 96-7.