
Abstract
The Expanded Program on Immunization (EPI) in India delivers vaccines under its policy, through government hospitals, health centers and outreach clinics. However, the national average full immunization coverage is stagnating at about 70%. The days and times of clinics are not always convenient for mothers working at home or employed outside. Moreover, vaccines not under EPI, but recommended by the Indian Academy of Pediatrics (IAP), are unavailable there, forcing mothers to go to private sector immunization clinics to get them. Recognizing the local need for user-friendly immunization clinic, we designed one in the Department of Child Health. The impetus came from local demand by a civil society organization (Rotary Club of Vellore). Our immunization clinic is open every working day (8.30 am to 4.00 pm) offering both groups of vaccines. Its success is illustrated by the fact that over 7000 children per month receive immunization in this clinic. We describe its design and operation so that this model may be replicated in other urban hospitals with pediatric sections.
Author Contributions
Academic Editor: Giuseppe Murdaca, Department of Internal Medicine-University of Genova, Genova , Italy
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Rajeev Z Kompithra, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
In India, many families obtain immunizations for their children through the Expanded Program on Immunization (EPI, also called Universal Immunization Program) in which specifically trained vaccinators immunize free of charge, in subcenters, primary health centers and community health centers. Pediatrics and/or Community Medicine Departments of Government Medical Colleges also provide EPI vaccines, mostly as part of outpatient clinics. Funds for staff salary, vaccines, cold chain, syringes and needles etc. are provided by the Government.
The EPI vaccines are BCG, OPV, Measles vaccine and Pentavalent vaccine (DwPT, HBV and Hib) 1. In a few states Measles, Mumps, Rubella (MMR) vaccine and in districts endemic for Japanese Encephalitis (JE), JE vaccine are also included 2, 3. Despite availability of free service, the average full immunization coverage nationally is hovering around 70% for several years 45, 6. Moreover, there is considerable disparity of coverage between states and within states between districts and within districts between urban and rural populations 4 6, 7.
Immunization sessions under EPI in health centers are usually once a week. In many Government Medical Colleges, even where outpatient clinics function daily, immunization is given only once or twice a week for a few hours, when outpatient service is suspended.
The operational constraints in both channels include competing demands for space and staff time between health care services and immunization. The barriers to achieve high immunization coverage through health centers include inconvenient locations and timings; long waiting hours; unwelcoming attitude of staff; occasional stock-outs of vaccines and absence of vaccinators and lack of systematic and organized health education 6.
In many private sector clinics and hospitals offering vaccines recommended by the Indian Academy of Pediatrics (IAP), the charges are often very high, even for EPI vaccines.
Immunization used to be given in our pediatric outpatient clinic during two afternoons per week. The clinics tended to be overcrowded with 200-300 mothers registering their children to be vaccinated during the short time of the clinic. Following a request and offer of support from a civil society organization (the Rotary Club of Vellore) to provide daily immunization service, in 1994 we opened the “Rotary-CMC Well Baby Clinic”, physically separated from the outpatient clinic and open 6 days a week.
Over the years, this clinic has grown in popularity. To illustrate, there were 89439 child-clinic-visits in 2014, inoculating various vaccines in 41038 children. The purpose of this paper is to describe the clinic in detail, in order to serve as a model.
Structure of the Immunization Clinic
The immunization clinic is located away from pediatric outpatient area where sick children are examined and treated, but within easy reach of the outpatient and emergency (casualty) clinics so that children needing attention can be referred and served with minimum delay.
The floor diagram showing the flow/movement of children is presented in Figure 1. The waiting area can accommodate 80 persons seated in queue. In the next room, children are registered and anthropometric measurements documented. Here 3 nurses are on duty; each parent is counseled regarding child health, growth, development, nutrition and immunization.
Figure 1.Floor flow diagram depicting the design of the clinic and movement of children
Next is the doctor’s room with one experienced pediatrician and a pediatric resident on duty. Each child is checked for growth and development and following a brief physical examination, vaccines are chosen after discussion and mutual approval between the doctor and the parent.
The next room has the payment counter where user fee is collected, consisting of cost of immunization card (one time), cost of vaccines, syringe, needles and service charges.
In the next room, all relevant data (vaccines, anthropometry) are registered in a data base. After these preliminary steps, inoculations are conducted in the Inoculation room where 4 nurses are on duty.
For breast feeding, mothers are free to sit in privacy in the adjoining room. All vaccinated children are required to stay in the premises for no less than 30 minutes and report to the staff any unexpected discomfort or symptom.
The inoculation room is equipped with an emergency trolley containing all necessary drugs and instruments for managing anaphylaxis [Bag valve masks, laryngoscopes and blades, blood pressure apparatus, stethoscope, torch light, Lignocaine jelly, Adrenaline, Calcium gluconate, Sodium bicarbonate, Dopamine, Midazolam, Atropine, Hydrocortisone, Dobutamine, syringes ranging from 2ml to 50ml,
arterial blood gas syringe, intravenous (IV) cannulas (24 G, 22G, 20G, 18G), Burette type metered dose infusion set, IV set, 3 way extension 10 cm, suction catheters (Nos. 8, 10), non-pyrogenic single dose containers with Normal Saline 100ml, 5% Dextrose 500ml, Compound Sodium Lactate 500ml and 10% Dextrose 100ml, Airway (0,1,2 size) and endotracheal tubes Nos. 2 to 7.5].
Vaccine Stock Management
Vaccines are procured by the hospital pharmacy department after Pharmacy Drug Committee approval. The pharmacy stores one month’s stock. The indented vaccines are supplied to the immunization clinic twice a week. The immunization clinic stocks one week’s supply. The vaccine store room in the clinic houses an Ice lined refrigerator and a domestic refrigerator. Vaccines for daily requirement are shifted into 2 refrigerators in the inoculation room. The inoculation room nurses maintain stock registers. All refrigerators are connected to regular as well as standby emergency power supply. During the night, in case any refrigerator gets no power supply, an alarm rings in pediatric casualty pharmacy services (manned 24 hours). The Pharmacy staff would notify the immunization clinic pediatrician in charge and senior nurse. They ensure the transfer of contents from the faulty refrigerator to the ILR or another functioning refrigerator within the clinic or if necessary, outside the clinic.
Range of Vaccines
We provide all vaccines recommended by EPI and IAP. From September 1999, we used a quadrivalent vaccine (DwPT+ Hib) either alone or in combination with Hepatitis B vaccine (HBV). From December 2002, we provide pentavalent (DwPT+Hib+HBV) vaccine.
We have introduced most licensed newer vaccines including MMR, Typhoid, Varicella, Hepatitis A, Pneumococcal polysaccharide vaccine, Meningococcal polysaccharide vaccine, Acellular pertussis containing vaccines – DaPT, Tdap and Pentavalent, Influenza vaccine (trivalent inactivated/ subunit), Inactivated polio vaccine, Rotavirus vaccine, Pneumococcal conjugate vaccine, Meningococcal conjugate vaccine and Human papillomavirus vaccine. Rabies vaccine is stocked and inoculated in Pediatric casualty.
Volume of Turnover
The annual number of children served, child visits, injections, OPV doses and Oral rotavirus vaccine doses inoculated from years 2003 through 2014 are presented in Table 1. A line graph showing the yearly growth trajectory of the annual numbers of children served, child visits, injections and oral vaccine doses inoculated from years 2003 through 2014 is presented in Figure 2.
Table 1. Annual Numbers of children served, child visits, injections, OPV doses and oral Rotavirus vaccine doses inoculated from years 2003 through 2014| Year | Number of children served | Number of child visits | Number of Injections | Number of OPV doses | Number of Rota virus vaccine doses |
| 2003 | 21248 | 46451 | 65729 | 36600 | - |
| 2004 | 22580 | 48101 | 68631 | 37080 | - |
| 2005 | 23231 | 49090 | 67307 | 40740 | - |
| 2006 | 24873 | 52383 | 68948 | 40080 | - |
| 2007 | 20660* | 54426 | 75002 | 44660 | - |
| 2008 | 26207 | 59255 | 89840 | 44740 | - |
| 2009 | 32128 | 67768 | 92057 | 49660 | - |
| 2010 | 35327 | 74583 | 100380 | 50380 | - |
| 2011 | 36164 | 75945 | 101804 | 50100 | - |
| 2012 | 35451 | 80248 | 112359 | 55490 | 107 |
| 2013 | 39837 | 82499 | 129732 | 51940 | 855 |
| 2014 | 41038 | 89439 | 145228 | 52200 | 6630 |
Figure 2.Line graph showing growth trajectory of numbers of vaccine doses given by injection, numbers of children and child visits, and vaccine doses given orally.
During 2014, the total number of vaccine doses inoculated was 204,058. Of these, EPI vaccine doses were 113,725 (55.73%) including OPV (52,200 doses), BCG (11,610 doses), DwPT and DwPT containing vaccines (27,114 doses of which 14,319 doses were pentavalent vaccine) HBV (14,063 doses), Hib (single dose-291 doses, total doses including as part of combination -24,888 doses), Measles (6379 doses), DT (220 doses) and TT (1848 doses) Figure 3. The number of newer, non EPI vaccine doses inoculated was 90,333 (44.27%). A pie diagram depicting the distribution of non EPI vaccine doses inoculated in 2014 is presented in Figure 4.
Figure 3.Pie chart showing the numbers of EPI vaccine doses inoculated in 2014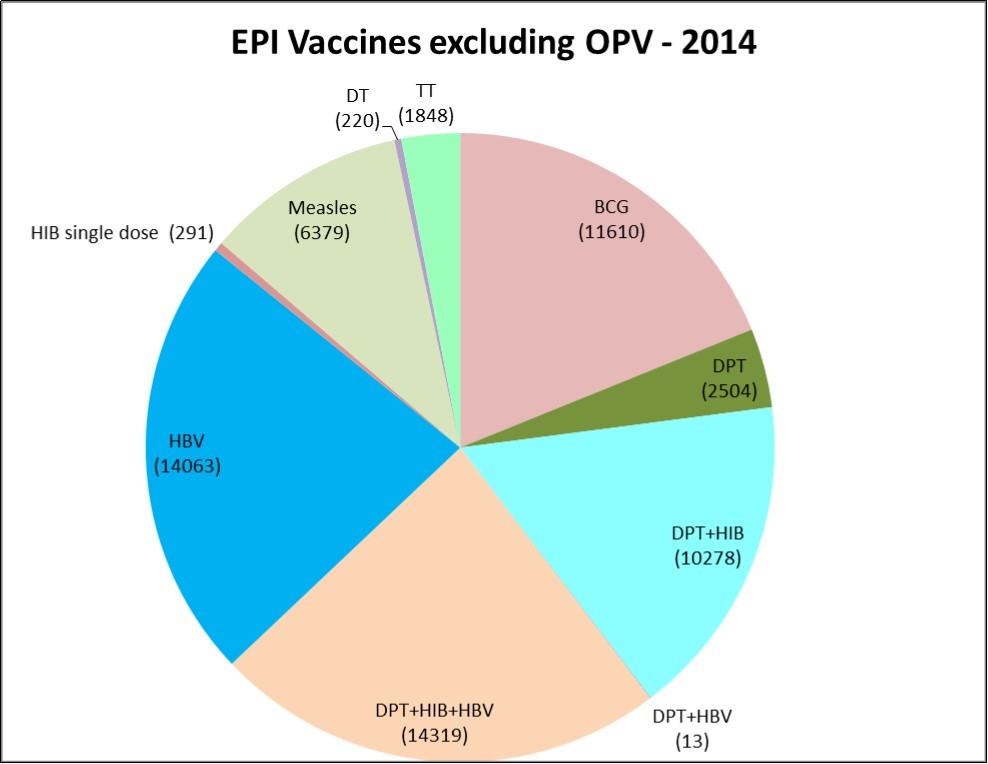
Figure 4.Pie chart showing the numbers of non EPI vaccine doses inoculated in 2014.
Discussion
The annual number of children served and the volume of vaccines given have steadily grown from the time this ‘franchise-like, cafeteria style’ clinic for immunization was opened. We charge a reasonable user fee including service charge (< $1) to cover overhead expenses and actual costs of vaccines, syringes and needles This may arguably be the highest volume immunization clinic, by way of volume of vaccines inoculated and number of children served, providingboth EPI and IAP-recommended vaccines, in India.
We present this success story in the hope that other medical colleges and hospitals with pediatric departments in India and other developing countries will replicate this model.
Parents come to know of this clinic by word-of-mouth conversations by satisfied clients who experienced user-friendly services. We have not advertised our services in any manner. Time of parents is saved by the institution agreeing to allow the Well Baby Clinic clientele to register in the clinic itself, without registering as hospital patients. Also, no mother needs to spend more than one and a half hour for the entire operations, on average, including 30 minutes of mandatory stay after inoculation.
Mothers are encouraged to bring children with any adverse reaction following immunization to the Well Baby Clinic, without delay. Such mothers do not have to join the queue, but are brought to the Pediatric officer after preliminary interview by the injection room nurse. When required, children are referred, accompanied by a nurse, to pediatric outpatient department, casualty or surgery for treatment and feedback. The common adverse reactions are fever, or pain and swelling at the injection site. Very rarely, we see injection abscess, about 2 per year. All adverse events (including febrile convulsions, hyperpyrexia, hypotonic hyporesponsive episode, persistent inconsolable crying as well as unrelated coincidental illnesses) are documented and reported to the Institution’s Quality Management Cell which conducts routine weekly quality checks.
In the last 20 years of this clinic’s experience, there has been no death as adverse reaction to any vaccine; we say this particularly because fear has been expressed that pentavalent vaccine causes child death8. We have given over 146,000 doses of pentavalent vaccine containing whole cell pertussis component since December 2002, and over 19,000 doses of pentavalent vaccine containing acellular pertussis component (DTaP, Hib, IPV) since January 2008, without any serious untoward after-effect (anaphylaxis or death). One reason for this safety record may be that every child is screened for any pre-existing illness or abnormality. When required, the immunization is postponed or conducted under observation by competent clinicians. For example, babies with congenital heart disease are immunized and observed in the pediatric clinic.
The families served by the clinic come from Vellore city and nearby areas 9. Unfortunately the Government EPI does not recognize this clinic as a channel for immunization, despite availability of computerized data, mainly because we are in the private sector and offer non-EPI vaccines. Therefore, the numbers of EPI vaccines given or children vaccinated (‘beneficiaries’ in EPI parlance) are not collected by District EPI Manager for immunization coverage calculations.
Such distinction between EPI and private sector immunization is artificial and unnecessary. Families of children immunized in our clinic usually keep the immunization card, as it is asked for whenever visiting the pediatric outpatient clinic; hence any household survey for immunization coverage can capture the information.
Conclusion
The Rotary-CMC Well Baby is a model for augmenting uptake of EPI and non-EPI IAP recommended vaccines in the community, evidenced by the large number of children served and the high volume of vaccines delivered. There are several barriers to achieving high immunization coverage in government centers despite the availability of free immunization services with EPI vaccines. Public demand for EPI as well as newer vaccines is high, with willingness to pay reasonable user fee for vaccines and services. If quality service is given during all working hours and if turnaround time is short, large numbers of families will avail of the opportunity. Thus, this is a replicable model.
Acknowledgements
We gratefully acknowledge the help and support of the Rotary Club of Vellore.
References
- 1.Gupta S K, Sosler S, Lahariya C. (2012) Introduction of Haemophilus Influenzae type b (Hib) as pentavalent (DPT-HepB-Hib) vaccine in two states of India. , Indian Pediatr 49, 707-9.
- 2.Bhatnagar N, Kaur R, Gupta M, Sharma D.Introducing combined measles, mumps and rubella vaccine in Chandigarh, India: issues and concerns. Indian Pediatr.2014Jun;. 51(6), 441-3.
- 3.Universal Immunization Program.Immunization Division at MoHFW. Universal Immunization Program (UIP) National Immunization Schedule (NIS). Available from: 4. National FamilyHealth survey 2005-06, India. Key findings from NHFS-3. NFHS-3 fact sheets for key indicators based on final data. Available from: http://www.rchiips.org/nfhs/factsheet.shtml Accessed onOct30,2015.
- 5.District LevelHousehold and Facility Survey 2007-08. India. Ministry of Health and Family Welfare Government of India. p90-97. Available from: http://www.rchiips.org/pdf/india_report_dlhs-3.pdf Accessed onOct30,2015 .
- 7.Annual Health Survey2012 - 13Fact Sheet. Census of India. Ministry of Home Affairs. Available from:.
Cited by (2)
- 1.Kulkarni Annarao, Holla Narayana, 2023, Should Every Medical College have a Dedicated Vaccination Clinic?, Healthline, 14(3), 171, 10.51957/Healthline_558_2023
- 2.Penugonda Asha J., Rajan Roshni J., Lionel Arul P., Kompithra Rajeev Z., Jeyaseelan Lakshmanan, et al, 2022, Impact of exclusive breast feeding until six months of age on common illnesses: A prospective observational study, Journal of Family Medicine and Primary Care, 11(4), 1482, 10.4103/jfmpc.jfmpc_1423_21